Employers Play Significant Role in Combating COVID-19 Misinformation
People who learn about vaccine safety and efficacy from employers are better at identifying misinformation and more likely to be vaccinated.

People who learn about vaccine safety and efficacy from employers are better at identifying misinformation and more likely to be vaccinated.

People who receive information about vaccine safety and efficacy from their employers are better at identifying misinformation and more likely to be vaccinated.
In the face of pandemic fatigue and gradual return to pre-pandemic levels of in-person events, travel, business operations and more, mistrust and misinformation around the COVID-19 vaccine threaten the prospect of sustainable pandemic recovery. Infection control measures such as sanitization and air filtration, while still critical to pandemic recovery and public health in general, have taken a backseat to vaccine and booster uptake as the primary driver of pandemic mitigation and abatement.
Employers are well-positioned to support health literacy and combat vaccine misinformation. Employers are increasingly many workers’ most trusted source for information as trust in government institutions, non-governmental organizations and the media has declined during the pandemic.
As vaccines became widely available in the U.S., followed by the necessity of boosters to maintain up-to-date vaccination status, the NSC SAFER team has monitored the role of employers in vaccine uptake and hesitancy through monthly surveys.
While many employers stop short of requiring proof of vaccination, the majority have implemented policies to encourage, assist or incentivize workers to get the COVID-19 vaccine. The SAFER team also monitored trends in vaccine uptake and employer policies with monthly surveys of 300 employers and 1,000 workers. It is consistently noted that sharing information about the COVID-19 vaccine and facilitating positive peer-to-peer storytelling about vaccination are associated with higher vaccination rates and significantly higher booster uptake, whether or not the employer requires vaccination.
This past March1, survey respondents who were not required to be vaccinated, but who had received information about the vaccine’s safety and efficacy from their employer had a 77.6% vaccination rate, while those who did not receive vaccine information at work had a 70.1% vaccination rate2. There is also a strong association between vaccine uptake and employer-facilitated positive peer-to-peer storytelling, with those workers having an even higher vaccination rate of 80.6%3. Booster uptake is especially high among this population when their employer had facilitated positive storytelling4.
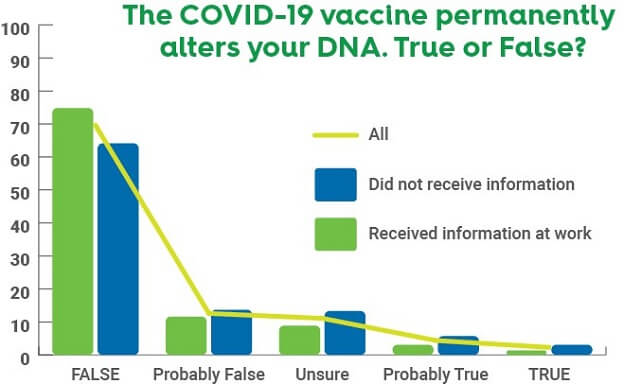
SAFER survey data find information sharing and employer facilitated Q&A sessions are strongly linked with workers being knowledgeable about the vaccine and better at identifying misinformation. Month after month, survey respondents who receive information from their employer are consistently more likely to answer correctly when asked to identify true and false statements about the COVID-19 vaccine. They are also less likely to answer “unsure,” on any true or false questions. The statements include factual statements about the vaccine interspersed with statements of misinformation. In responses collected March 23-28, 2022, respondents who received information at work identified, on average, true and false statements correctly 75% of the time, while those who did not only identified 57% correctly.
It is also important for employers and researchers who study health literacy to note there are two distinct types of misinformation: misinformation and blatant disinformation intentionally spread to obfuscate the truth about vaccination. This suggests hypotheses on how different types of misinformation are affected by employer policies. While perhaps not entirely distinct, misinformed beliefs can be driven by two things. The first is a lack of knowledge about how vaccines work, which leads to misunderstandings and is associated with lower health literacy. The second is disinformation intentionally pedaled by anti-vaccination influences fueled by a mistrust of science and medicine.
More common statements that may be believed simply due to a lack of understanding include the notion that vaccinations alter your DNA and whether antibodies can be passed to babies via breastmilk and offer infants some protection against infection. These are possibly easier to correct because they are misunderstandings, as is the concern of whether the vaccine will come with an out-of-pocket cost.
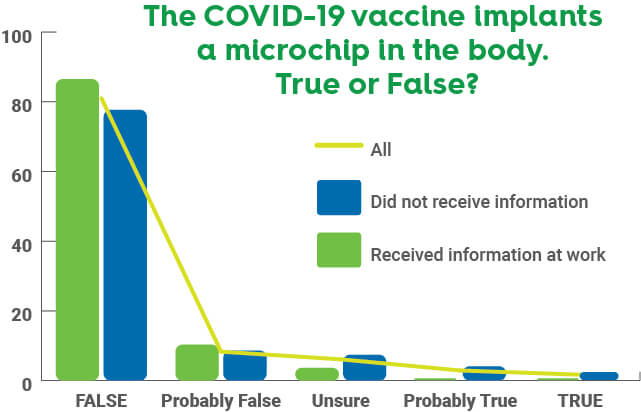
The association between workplace vaccine information and vaccine knowledge was present even when it came to the more outlandish claims that very few respondents endorsed. This type of misinformation, such as the vaccine implanting a microchip tracking device, are often asserted by influential purveyors of disinformation and shared within social media groups, including private conversations, which aren’t subject to oversight and fact-checking by the media platform. For this reason, they can be more “sticky” forms of misinformation to combat. Additionally, once a person starts to believe a myth rooted in distrust of science, they are unlikely to change their mind based on evidence.
Many survey respondents who received information about the vaccine’s safety and efficacy also said they had received information such as how and where to schedule appointments and other logistical factors. These respondents were less likely to report that finding a convenient location to get vaccinated was a barrier to access for them, and more likely to know definitively whether people without health insurance have to pay out-of-pocket for the vaccine.
As employers are increasingly the most trusted, and most effective source of information for workers, the SAFER project suggests employers consider the following actions to help quell vaccine hesitancy and counter misinformation workers may receive outside of work from less-than-reputable sources:
● Provide fact-based, unbiased information to their workers from reliable sources such as the CDC
● Facilitate Q&A sessions between medical professionals or vaccine experts and employees
● Facilitate positive, peer-to-peer storytelling among employees about vaccination in a safe, non-judgmental environment
● Provide information in the primary language of all workers in a multi-lingual workforce
As always and throughout the pandemic, the SAFER team is here to support employers and workers as we enter the next phase of COVID-19. If you have any questions about the effort, or about getting involved, please contact us at [email protected] to reach Program Manager Stephanie Roberts, Research Associate Caitlin Lang and others who can provide more resources and address further questions.
We hope employers will keep actively engaging with the SAFER team as we continue our efforts to provide data-driven resources, guidance and solutions to the business world.
1Data collected March 23-28, 2022, from 1,001 people who currently work for wages as employees or contractors and are not self-employed. A representative sample of the U.S. workforce was obtained through a national polling firm. The demographic characteristics of survey respondents was consistent with those of the U.S. workforce. Full demographics are listed in the methods tab below.
2The vaccination rate was significantly different between groups as assessed by Chi-square test of association, X2 (1, n = 700) = 4.944, p = .026
3The vaccination rate was significantly different between groups as assessed by Chi-square test of association, X2 (1, n = 610) = 7.16, p = .006
4Of fully vaccinated respondents without a vaccine requirement, 63.2% had already received a booster, while that rate was 70.8% for people who had experience positive peer-to-peer storytelling at work, and 60.1% for those who did not, X2 (1, n = 495) = 5.047, p = .025
The SAFER Workforce Trends Indicator Survey is a survey distributed monthly in order to track trends among the workforce related to COVID-19 at work, and their attitudes toward vaccination and employer policies. The survey questions and methods are approved by the Institutional Review Board of the National Safety Council. Respondents can opt to exit the survey at any time with penalty.
The survey is distributed through a nationwide market research and opinion polling firm to a participant pool who can voluntarily opt in to participating in the study. Respondents complete the survey on their personal computer or mobile device, and are compensated for their time.
The survey is built in Qualtrics, and quotas are enforced in order to ensure the demographics of the respondent pool reflect approximately the demographic make-up of the American workforce. Respondents are people who currently work for wages as employees or contractors and are not self-employed.
Demographics
Participants were adults aged 18 to 65 who are currently working for wages. The mean age of participants was 47.8, and 49.2% were female.
Margin of error for the total sample size was +/- 3% at the 95% confidence level. Statistical analyses are performed using IBM SPSS Version 22.

With a century-long legacy, the National Safety Council is a global center for safety expertise. Let's work together to align resources. We look forward to learning about ways we can join efforts to expand safety everywhere!
There are no items in your cart